


Genome #7: Towards better healthcare enabled by stronger political competition
More healthcare centers ≠ Better healthcare

Cast iron law of politics is that politicians like to be re-elected.
In the “political market”, the politician (provider) and the voter (receiver) are often on unequal footing: 1) the voter has limited information about how the politician has really performed beyond what is visible (and measurable) and 2) identity-based politics (preference of the voter to vote for a politician from their religion or caste).
Are poor health outcomes in countries always a result of a lack of resources?
In developing countries, healthcare provision is often “public” - provided for by the government, at least in part if not whole. This encompasses not only “public health” (the science and art of preventing disease, prolonging life, and promoting health) but also healthcare facilities. Providing for public health has huge positive externalities - for example, vaccinating a part of the population against an infectious disease not only keeps them safe but also prevents the spread of infection. As such, government interventions in public health and healthcare are targeted at increasing overall welfare. The government is well aware of the huge positive externalities, the voter will only benefit from it - then why are we still living in times of poor health outcomes? For some context, India’s health care system performs worse than its low- and middle-income peers - in 2019, India had a Disability Adjusted Life Years Rate (DALY Rate - number of healthy life years lost due to premature mortality per 100,000 population) of 33,643 with a PPP (Purchasing Power Parity) adjusted GDP of $6,997 compared to Bangladesh’s DALY rate of 27,077 at $4,964 PPP GDP.
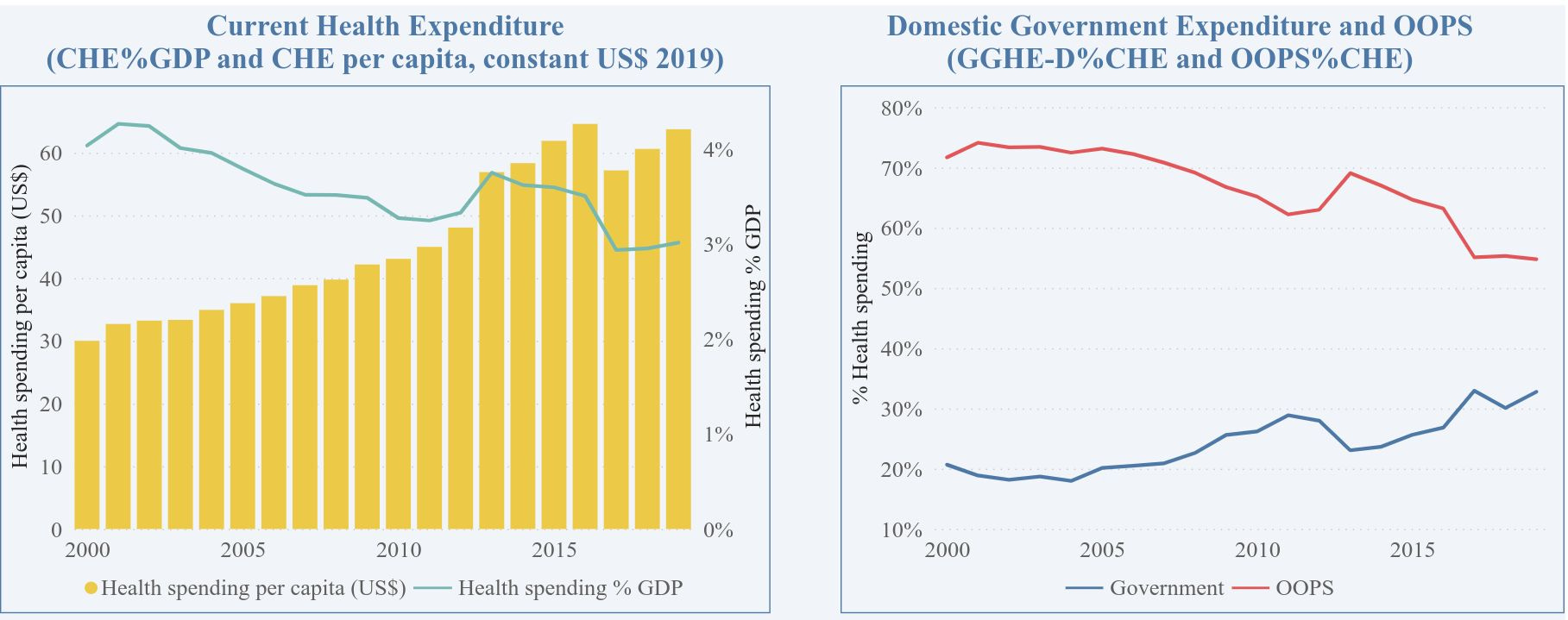
It is easy to argue that our poor health outcomes are a result of lack of investment and efficiency, leaks, and general lack of resources. For example, the Indian government spends around 1.18% of GDP on health while overall we spend around 3.84% on health - implying the remaining 2.7% is borne as out-of-pocket expenditure by the voters (the share of insurance companies is much smaller).
There is another viewpoint that explains the inadequacy of our healthcare system - we never demand it! In the post-poll survey conducted by Lokniti-CSDS (2019 elections), the top issue for 14.3% of voters was development followed by unemployment, price-rise, and corruption while only 0.3% of voters prioritized the conditions of health care facilities.
What happens when there is more competition? → We have more health centers but with no facilities
Elections provide a wonderful opportunity for voters to hold politicians accountable - the incumbents have a chance of re-election if they are competent (in theory) or be driven out of office. For a rational voter not driven by personal biases (of caste/religion or other marginalizing factors), the assessment of a politician is based on information cues that are (easily) accessible or visible. On the other hand, a politician is responsible for allocating the limited resources he/she has access to, towards activities that above all ensure that he/she gets re-elected (see Besley’s cast iron law1) while possibly maximizing public welfare. The politician provides cues to the voter through these activities, particularly more so when the election is competitive.
How do the politicians get away with neglecting health care in all the elections? What do we, the voters, really think before voting? Our thought process is driven by what we really see around us - information that is within our reach. For example, a new hospital in our constituency is a visible cue and has little cognitive deliberation necessary. However, obtaining information about whether there is a functional X-ray machine and a qualified operator is costlier (and almost impossible) to obtain for the voter. When obtaining information requires substantive cognitive deliberation, the instinct of the voter is to remain rationally ignorant and use information shortcuts2 Healthcare is full of information friction - we can “see” the hospital, but it is almost impossible to assess its facility-level capacity (how many doctors/nurses/staff, which facilities exist and are operational). As such, the hospital here becomes a visible good with the easiest cue possible. Thus, a politician who provides for a new health care center might be rewarded by its voters, who tend to discount the provision of other goods such as the doctors or facilities available at these centers because of the information barrier driving them to be rationally ignorant. A wonderful paper from Subham Kailthya and Uma Kambhampati found that an increase in political competition raises the probability that a village will have a health facility by 8-15% but does not significantly affect the provision of (even) inexpensive supplies at these facilities. So the poor healthcare outcome is not merely a result of lack of health centers, but whether the existing ones are operational in a true sense.
What is the solution?
Having electoral competition forces the incumbents to give out visual cues to the voters. We need a stronger auditing system that will ensure that the health centers are truly operational. The information barrier arising from the huge friction in assessing the facilities of these centers can be reduced by making this information readily available on the district health officer’s website. Yeh public hai, sab jaan hi jaati hai.
Downs, 1957 An economic theory of democracy