I went for my routine annual physical exam in May 2023. Everything was normal, I felt the usual. My reports arrived a day later. Most things looked okay but a few markers were up. I was in the middle of a job search and that used to keep my mind occupied all the time. So when the reports came, I was not bothered. I did not care to understand what these values meant. Two days later, my physician typed in her analysis of the report:
Blood sugar: normal but if it goes any higher, it will be pre-diabetes. So, work on healthy diet, exercise, and weight. Blood chemistry: normal. Cholesterol: HDL (good cholesterol) is low. Increase it by increasing regular exercise. Triglycerides are very high. Improve it by avoiding products with white sugar/flour. Non-HDL cholestrol is high. Limit saturated fats and processed food. Repeat lipid profile. We might have to put you on statins.
As any physician would tell you, the numbers on this report are concerning (particularly more so for a person my age) and I have no inhibitions talking about them here because these numbers would take me on a journey of understanding how far your dreams, inspiration, instincts, hard work, and grit take you sometimes.
My lipid markers were way too off for someone my age. I was living a very unhealthy life - too much stress and almost zero physical activity barring the joyful walk from the ribs of WTC station to my office and back. Every Friday, I would have a large pizza or a potful of biryani. It was the end of the week after all.
My reports from just a year back, in June 2020, were almost perfect. A lot had changed in one year. I blame the pizzas mostly - they were not my favourites anyway. Pizza also ticked all the checkboxes the physician was asking me to avoid: sugar + white flour + saturated fats. But that is not what I want to talk about.
I want to talk about statins. I was curious. What would statins do? Why was the physician recommending a drug over lifestyle changes?
“Are statins safe”? I asked her.
“They are very safe and extremely effective at preventing cardiac attacks. They are so safe that we should just put them in our piped drinking water so everyone remains safe!”
That’s a very bold claim. I ignored her mostly but did read up on statins. The story of the discovery of statins, (one of) the wonder drug, is of dreams, inspiration, instincts, hard work, grit, andloss.
“Why are we considering statins?” I followed up.
“Your ‘bad’ cholesterol is high, your ‘good’ cholesterol is low. This puts you at a danger of developing plaques in your arteries. If we don’t address the problem, you will be at a risk of a cardiac arrest”.
Statins are often considered one of the most significant medical discoveries since penicillin, the original wonder drug and the most widely used antibiotic. But what exactly do statins do? Simply put, statins are a class of drugs that help prevent heart attacks by reducing the build-up of your low-density lipoprotein (LDL) cholesterol, often dubbed as the ‘bad’ cholesterol.
Cholesterol - the Janus particle
Cholesterol is the most highly decorated small molecule in biology. Thirteen Nobel Prizes have been awarded to scientists who devoted major parts of their careers to cholesterol. Ever since it was isolated from gallstones in 1784, cholesterol has exerted an almost hypnotic fascination for scientists from the most diverse areas of science and medicine.... Cholesterol is a Janus-faced molecule. The very property that makes it useful in cell membranes, namely its absolute insolubility in water, also makes it lethal”.
— Michael S. Brown and Joseph L. Goldstein, Nobel lecture, December 1985
Janus was a two-faced god, in Roman mythology, who was a doorkeeper of heaven. He is two-faced with one face looking into the past and one face looking into the past. He is the guardian of the beginning and the end. It is January, the month of looking forward and reflecting on the past. What has cholesterol to do with Janus?
Cholesterol, like Janus, is a double-faced molecule. On one face, it acts as the building block of many crucial elements the body needs. On its opposite face, it acts as the lethal molecule responsible for forming plaques on the surface of arteries (and hence often dubbed as the “bad” cholesterol) subsequently leading to coronary heart disease.
Cholesterolisvital to our existence. The most common steroid in the body is cholesterol. The brain constitutes just 2% of your body weight but holds 20% of the body's total cholesterol! Cholesterol is also necessary for digestion - it produces bile acids that digest fats in our food. Cholesterol is a building block for synthesizing sex hormones - cholesterol in the testes gets converted to testosterone and cholesterol in the ovaries is converted to estrogen.
In 1964, the Nobel Prize in Physiology or Medicine was awarded to Konrad Bloch and Feodor Lynen for discovering the mechanism of cholesterol and fatty acid metabolism. The same year, Dorothy Hodgkin won the Nobel Prize in Chemistry for her work on “determinations by X-ray techniques of the structures of important biochemical substances”. Her first structure, in 1943, was of a cholesterol (iodide).
Your discoveries may provide us with weapons against some of mankind’s gravest maladies, above all in relation to cardiovascular diseases. Achievements like yours make it not unrealistic to look forward to a time, when mankind will not only live under vastly improved conditions, but will itself be better.
— Rector Friedberg to Dorothy Hodgkin, Konrad Bloch and Feodor Lynen in the 1964 Nobel Banquet
British commemorative stamp celebrating Dorothy Hodgkin’s work. Courtesy: Royal Society
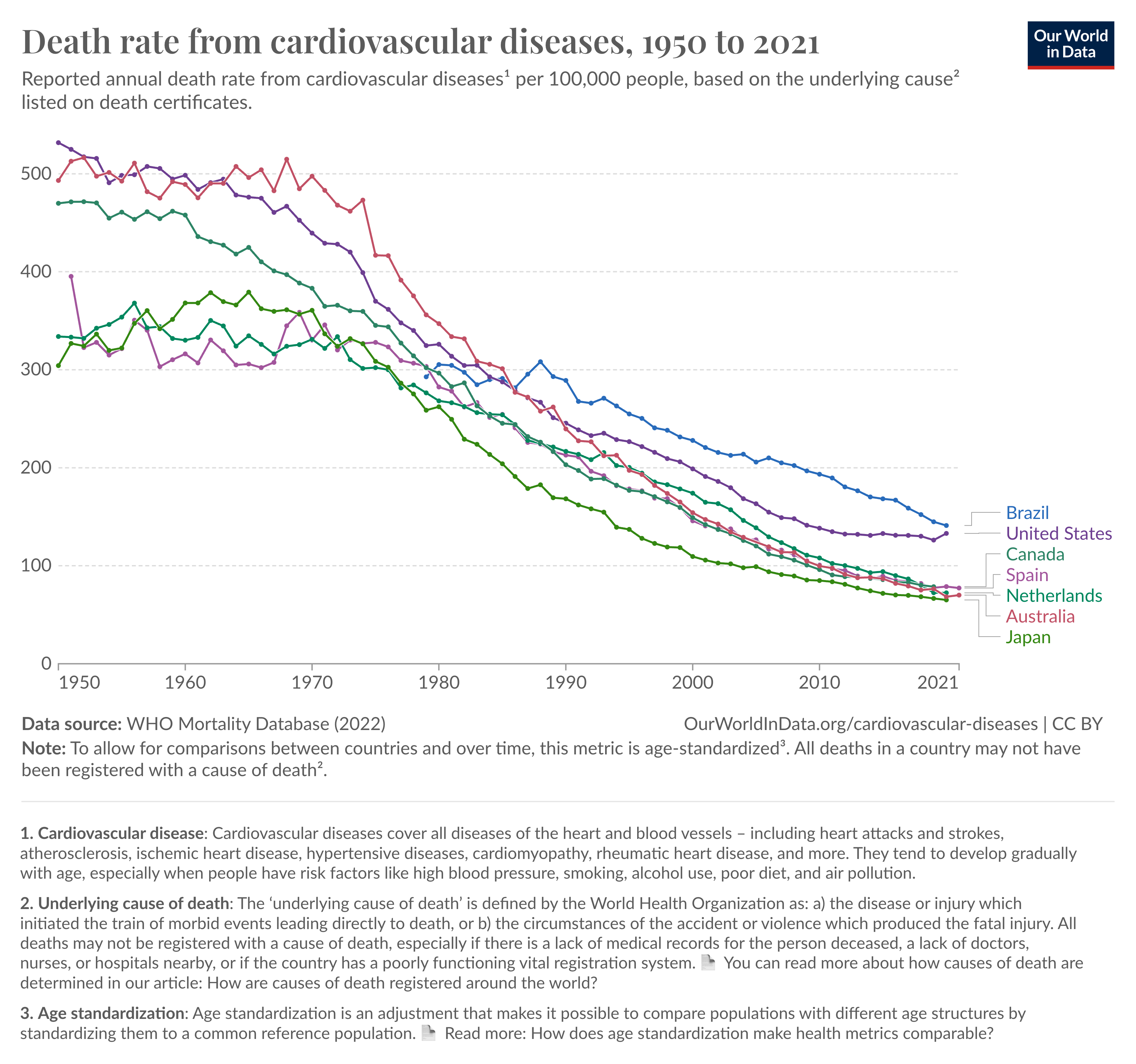
Rector Friedberg’s 1964 predictions came true. In the following decades, science made tremendous progress in understanding the root causes of cardiovascular deaths and began targeting these causes one by one. A major breakthrough in this effort was the development of statins.
The scientist dream
The story of statins is the story of Dr.Akira Endo. I will take the liberty of referring to him by his first name. Akira was born in 1933 in a rural farming family in the small town of Yurihonjō (Akita) in northern Japan. He lived there with his extended family including his grandparents. Endo’s grandfather had an interest in medicine and science and was his home teacher, who gave him his first exposure to science. When Akira was just 10, he dreamt of being a scientist. He was inspired by Hideyo Naguchi, a Japanese scientist who went to the United States and discovered the bacterial agent causing syphilis.
While doing a bachelor’s in Agricultural Sciences at the Tohuku University’s College of Agriculture in Sendai, Akira read the biography of Alexander Fleming who discovered the “first wonder drug” penicillin in 1928. Penicillin is an antibiotic - it kills bacteria. Produced by a mould or fungus (Penicillium), penicillin’s discovery is a story of serendipity and warrants a digression.
Fleming discovered penicillin while investigating staphylococcus, a common type of bacteria that causes boils and severe infection in people with weak immune systems. In 1928, Fleming took a two-week vacation. He left his petri dish where he would grow his bacterial colonies on his lab bench. When he came back, he found a mould growing in the petri dish. There was also bacteria on that dish but none surrounding the mould. The mould in its periphery had overpowered the bacteria. The mould had found its way into the petri dish by chance - either through a window Fleming left open or probably floating up the stairwell from the lab which used to culture various moulds. Penicillin had been discovered serendipitously. A decade later, Penicilin would save thousands if not millions of lives during World War II. Akira was influenced by Fleming’s discovery of the moulds which demonstrated that a fungus could act as a powerful pharmacological agent.
For Akira, Fleming was his“religious inspiration”. While serendipity played a crucial role in Fleming's discovery, Akira chose not to rely on chance. Instead, he achieved remarkable success through hard work and determination. He also advised students to follow this approach:
The advice I would give to students interested in pursuing research as a career is to have big dreams and goals and to work hard towards them.
After graduating from college in 1957, Akira joined a pharmaceutical company Sankyo in Tokyo. His first assignment was to develop an enzyme that could break down pectin (fibre in the fruits) which would otherwise make the wine pulpy and hazy. The very next year, he found a fungus (Coniothyrium diplodiella) parasite, that often infects grapes, to be a viable source of the required enzyme. One more year later, the enzyme was commercialized promising everyone non-hazy non-pulpy wines!
At some point, Akira got interested in cholesterol biosynthesis. The Nobel Prize awarded in 1964 to pioneers of cholesterol biosynthesis provided the push he needed In 1965, he wrote to Harvard University’s Konrad Bloch, one of the two Physiology prize laureates (the other laureate was Feodor Lynen a German and Akira, inspired by Hideyo probably only wanted to come to the US), asking him to be his postdoc advisor (Akira had just finished a PhD In Biochemistry from Tohoku University in 1966). That request did not work out, so Akira went to work with the biochemistry department with Lawrence Rothfield at the Albert Einstein College of Medicine in New York City from 1966 to 1968. Rothfield had worked as a physician for New York University. It was from Rothfield that Akira first learned about “hypercholesterolemia” (high levels of cholesterol in the blood) being a major risk factor for coronary heart disease which was the No. 1 killer disease in Western countries. These two years in the US were instrumental in pushing Akira to think about the actual problem he was about to solve. Akira writes:
While living in New York, I was very surprised by the large number of elderly and overweight people, and by the rather rich dietary habits of Americans compared to those of the Japanese. In the residential area of the Bronx where I lived, there were many elderly couples living by themselves and I often saw ambulances going to take an elderly person who had suffered a heart attack to the hospital. At that time, coronary heart disease was the main cause of death in the United States. The number of patients with hypercholesterolemia, a precursor to coronary heart disease, was said to exceed 10 million
The rate-limiting step
One of the initial core courses in my Chemical Engineering curriculum was ‘Chemical Reaction Engineering’. Mastering reaction engineering entails grasping two fundamental aspects: reaction kinetics and reactor vessel design. In reaction kinetics, a key takeaway is that to maximize the yield of a reaction, you must optimize the rate-limiting step—the slowest stage of the process. This advice is also generally applicable, though I don't want to digress.
Cholesterol synthesis involves several steps and primarily happens in the liver. The rate-limiting step in the pathway is the synthesis of HMG-CoA (3-hydroxy-3-methylglutaryl coenzyme A) from acetyl-CoA. If the name sounds like a mouthful, the flowchart below could help. This conversion is facilitated by an enzyme called (unsurprisingly) HMG-CoA reductase. It is called so because it carries out a reduction reaction. You probably studied reduction reactions in your high school but the details do not matter here.
The cholesterol pathway
If you want to slow down cholesterol synthesis in the liver, inhibiting HMG-CoA reductase is the optimal and safest strategy. It is optimal because HMG-CoA reductase is the rate-limiting factor in cholesterol synthesis. It is safest because several intermediate compounds are synthesized between acetyl-CoA and cholesterol. Targeting HMG-CoA reductase helps ensure no secondary buildup of these compounds, which might induce toxicity.
Inspiration takes one step forward
After a productive two-year stint in New York, Akira returned to Sankyo in 1968 and was allowed to work on a project of his interest. Numerous studies had shown that antibiotics can inhibit enzymes not only in bacterial cells but also in mammalian cells (penicillin kills the bacteria but not the human host). Akira had a hunch: if he could find a mushroom or a mould (fungi) that could inhibit the HMG-CoA reductase enzyme, he would hit the jackpot. Akira talks about his hunch in an interview:
The research was very high-risk and there was no guarantee we would find one. But I had a feeling that we would find it if I check through thousands of fungi.
Why would fungi produce anything that affects HMG-CoA reductase and that too in a mammal? Was Akira grasping at straws? Fungi need to evolve defences against all sorts of microbes. They would need to attack microbes that require sterols or other related products for their growth, and it was possible that these fungal compounds could also inhibit HMG-CoA reductase.
Reading the biography of Fleming played a crucial role in Akira’s next steps at Sankyo. Inspired by Fleming’s success in synthesizing antibiotics from fungi, Akira’s group began culturing thousands of fungi in 1971, hoping that one of them would effectively inhibit HMG-CoA reductase. One year and 3,800 strains of fungi later, they found a potent strain that significantly inhibited HMG-CoA reductase activity.
A compound active against sterol biosynthesis was isolated from the culture filtrate of the fungus Prthium ultimum IAM 6073 and identified as citrinin which had been isolated as an antibiotic.
The fungus, Prithim ultimum, was synthesizing citrinin, an antibiotic discovered in the 1930s. Akira's group demonstrated that this previously known compound could inhibit HMG-CoA reductase and lower serum cholesterol levels in rats. This could have marked the arrival of a new wonder drug, but it wasn't to be—citrinin was toxic to the kidneys. However, this discovery provided hope that antibiotics could be effective against cholesterol.
‘Gritting’ through the wonder blue-green mould
In the summer of 1972, after screening 6,000 strains of fungi, Akira and his group came across a culture broth of a blue-green mould, Penicillium citrinum Pen-51. Pen-51 had been isolated in the 1960s as a blue-green mould growing on rice from a vendor in Kyoto, where Akira’s laboratory was located. Pen-51 was a promising candidate as it could inhibit cholesterol synthesis by inhibiting HMG-CoA reductase in a variety of cultured cells. In July 1973, Akira’s group isolated the metabolite responsible for this inhibition and named it ML-236B, later known as compactin. Following in Alexander Fleming’s footsteps, whose discovery of penicillin came from the same genus, Akira’s discovery was the result of hard work and grit, rather than serendipity.
Penicillium citrinum Pen-51, the fungus that produces compactin statin. Source
Akira’s team showed that compactin, the first statin to be discovered, strongly inhibited the synthesis of cholesterol from acetyl-CoA in cultured mammalian cells. They also showed that if you cultured cells from patients with hypercholesterolemia, compactin could reduce the cholesterol levels by 50%.
Statins like compactin act by inhibiting the activity of the enzyme HMG-CoA reductase.
Rats almost kill the drug
In 1974, biologists at Sankyo started evaluating the efficacy of compactin by feeding rats a diet with supplements of compactin. After 7 days, there was no reduction in serum cholesterol. Two years of work and 6000 tests had vanished and the rats were to be blamed!
Akira’s team continued their efforts to elucidate what was going wrong in rats but not in cultured human cells. While there was no reduction in serum cholesterol levels after giving compacting for 7 days repeatedly, a single dose of compactin was effective in lowering serum cholesterol levels between 3 and 8 hours. After 8 hours, the liver (the primary organ where cholesterol is synthesized) in rats would start producing more HMG-CoA reductase and so if compactin was given repeatedly, the HMG-CoA reductase quantity would have increased 8-10 fold thereby cancelling out any inhibition of cholesterol synthesis by compactin.
In 1976, Akira found Noritosh Kitano, a pathologist at Sankyo who was using egg-laying eggs for his research. Kitano gave some of his hens for a compactin trial. Akira’s team showed that the plasma cholesterol in egg-laying hens could be reduced by 34% with a compactin supplement after 2 weeks. They went to show its efficacy in dogs and monkeys. Compactin was a gold candidate for being the drug for preventing cardiac arrest - the wonder drug. In August 1976, the “Compactin Development Project” started with Akira and his team of pharmacologists, pathologists, toxicologists, organic chemists and microbiologists.
A second problem would soon arise with rats just 8 months after the launch of the Compactin Development project in April 1977. The toxicologists reported that rats who had been fed high doses of compactin (500 milligrams per kilogram body weight per day mg/kg/day) ended up with crystalline structures in their livers which were believed to be toxic. In the next 9 months, Akira’s team proved that these crystalline structures were non-toxic cholesterol.
The fate of compactin and stealthy trials
Sankyo’s management was unenthused in pushing compactin for a drug trial even after the promising results of cholesterol reduction in humans, dogs and monkeys. The odds of success in making a drug even today remain low for a drug with a new mechanism. instead, Sankyo management decided to maximize their odds by focusing on a drug with a somewhat proven record - fibrates.
Without support from management, Akira Endo tried something that would absolutely not be allowed today. With support from his direct supervisor, Dr. M Arima, Akira initiated clinical trials in humans, stealthily. He initiated a study with a physician Dr. Akira Yamamoto at Osaka University. In February 1978, Yamamoto started treating an 18-year-old woman with hypercholesterolemia with compactin. This would have been impossible in the current times without applying for an Investigational New Drug or similar application to the regulatory agency.
Yamamoto gave a strong dose of compactin and the 18-year-old girl experienced muscle weakness which could be reversed by discontinuing compactin. Even after being discouraged by authorities at Osaka University, Yamamoto, secretly, gave compactin to five other patients and they all observed a cholesterol drop of 30% of the average with no adverse side effects. They published these results, setting the stage for a Phase 1 clinical trial to commence. Parallelly, this also initiated long-term safety studies in dogs for assessing the impact of compactin over a longer duration.
Sankyo initiated Phase 1 trials among patients with severe hypercholesterolemia. However, by mid-1980, these trials had to be halted. It wasn't due to issues with the patients or the trial itself, but rather problems arose in the long-term safety studies. Compactin, the pioneering statin, would never return, at least not commercially.
Dogs kill the drug because the drug kills the dogs
In 1978, Akira retired from Sankyo and in January 1979, joined Tokyo Noko University as a Professor. In August 1980 in a meeting with physicians involved in the compactin trials, Sankyo decided to permanently suspect the development of compactin which had been moving smoothly. The detailed reasons for this suspension were never communicated. But it was probably the dogs - they were dying. The 2-year-long toxicity trials in dogs had been given 100 or 200mg/kg/day of compactin and they had begun to develop lymphomas. The prescribed dosage for most statin therapies remains 10 or 20mg once a day. These results were never published and so academically speaking they were just rumours. The rumour of the dogs dying killed compactin forever.
The bigger fish establishes its dominance
Toward the end of the 1970s, inspired by the promise of leveraging fungi to produce HMG-CoA reductase inhibitors, and the trials showing the toxicity of compactin in dogs, pharmaceutical companies began searching for another statin.
In 1976, Merck Research Laboratories signed an agreement with Sankyo to give Merck access to its data and method connected with Akira’s compacting. Why would one pharma company sign an agreement with another pharma company? It is not unusual for companies to release such information to potential business partners to explore but this agreement wasn’t a fair one — Merck did not owe Sankyo anything if it found any other statin-like product in a different fungus. As fate would have it, that is exactly what happened. In February 1979. Merck isolated a statin very similar to compactin in chemical structure - called mevinolin from the fungus Aspergillus terreus.
At Tokyo Noko University, Akira continued his work on reductase inhibitors where in February 1979 he identified another statin, monacolin K, from a fungus Monascus rubber. In the fall of that year, it was shown that monacolin K and mevinolin were the same compound. Monacolin K and mevinolin would be called lovastatin.
In April 1980, Merck began preliminary clinical studies of lovastatin. Five months later, in September 1990, it discontinued the trials because of rumours that compactin (the original statin that Akira discovered) was killing the dogs by inducing big tumours. The lovastatin project was dead by the end of 1980. Roy Vagelo writes
September 1980. I made the decision to discontinue clinical trials of lovastatin because of rumors (to this day never substantiated) that the closely related compound, compactin, caused certain cancers in dogs. Nothing we had seen with lovastatin had given us any cause for concern, but we could not ignore the rumors about a chemically related HMG-CoA reductase inhibitor. It appeared that the lovastatin project was dead.
In January 1981, a series of results would seal the fate of statins. Brown and Goldstein, who would go on to win the Novel Prize in Physiology or Medicine in 1985, published a report showing that lovastatin reduced LDL cholesterol in dogs. Eight months later, in August 1981, another reportshowedcompactin successfully reducing cholesterol by 30% (with no fall in HDL cholesterol) in severe patients with hypercholesterolemia. This report would give statins, and specifically lovastatin a second life.
In 1984, Merck restarted large-scale clinical trials of lovastatin in high-risk patients. Merck also restarted the long-term toxicity studies in dogs that had previously only delivered rumours. These trials delivered two main results 1) lovastatin (or Mevacor, the commercial name) reduced cholesterol levels in patients with no significant side-effects and 2) dogs did not get tumours. In November 1986. Merck submitted its New Drug Application to the U.S. FDA. By September 1987, lovastatin (Mevacor) would have the FDA approval making lovastatin the first commercial statin on the planet. The global market for lovastatin is currently valued at nearly one billion US dollars.
Sankyo would go on to develop a second statin, called pravastatin (synthesis from the urine of dogs who were fed compactin) without Akira around, and would avoid the trouble created by the dogs by limiting the dosage to 25mg/kg/day (same as what Yamoto had found to be safe in humans). Bristol-Myers Squibb marketed and sold pravastatin as Pravachol after its FDA approval in 1991.
By 2001, the world will see six statins in the 10 billion US dollar market: Pravachol (pravastatin), Mevacor (lovastatin), Zocor (simvastatin), Lescol (fluvastatin), Lipitor (atorvastatin) and Baycol (cerivastatin). Compactin missed the bus and had long been forgotten.
The loss
Despite pioneering the field of statins and working on it passionately, Akira Endo did not receive the recognition he deserved for his groundbreaking work.
Akira Endo wasn’t one among “the thirteen noble prize winners who devoted major parts of their careers to cholesterol”. In 2008, at the age of 74, he was awarded the “America’s Nobel” prize, the Lasker Award. In 2017 he won the Gairdner Award for “discovering the first statin drug, compactin, and demonstrating its clinical efficacy”.
On June 5th, 2024 at the age of 90, Akira Endo, died leaving behind a legacy that will keep aspiring future scientists believing in their dreams and working hard! Akira would never win a Nobel Prize.
What goes around comes around
A WSJ article written in 2006 claimed Akira himself avoided taking statins even when his cholesterol levels were high:
At his checkup in 2004, his LDL, or "bad" cholesterol, was 155, a level at which many U.S. doctors would prescribe a statin. Dr. Endo says he didn't take anything and brought the number down to 130 last year by exercising more. Why would the inventor of statins bypass his own invention? Dr. Endo can only cite a Japanese proverb, "The indigo dyer wears white trousers."
Today I have good news and bad news. The bad news is that my cholesterol levels have reached 240 mg/dl. Maybe I had Sukiyaki or Shabushabu too often! And the good news is I can finally test a statin drug on myself. We might see soon how it works. And the funny thing is that the doctor said “Don’t worry! I know some very good drugs to lower your cholesterol”. Obviously, he did not know who I was.
In 2017, Akira finally told the world that both he and his wife were on statins, after all, “what goes around comes around”.
The effectiveness of statins has been proven by 25+ randomized placebo-controlled trials involving 200,000+ middle-aged followed for 5 years. Results in most studies are consistent: statins reduce “bad” LDL cholesterol by 30% and thereby saves lives of those who are at risk. There are no free lunches - the claim of statins being as safe as they should be supplied in our pipe drinking water does not hold up. There is enough evidence to show statins can induce muscle pain and put you at an increased risk of diabetes.
I will leave you with a simple correlation plot, as an exercise. The plot shows cardiovascular (more specifically due to Ischemic heart disease) death rates across different European countries on the Y-axis and statin use on the X-axis. What is your interpretation?
Disclaimer: The content provided in this post is not intended to be a substitute for professional medical advice, diagnosis, or treatment of any disease. Please seek the guidance of your physician or other qualified health provider.
P.S. I am on statins.
Thank you for reading Genome of India. This post is public so feel free to share it.






{kind=link}


{kind=link}
#/media/File:Akira_Endo_cropped_3_Akira_Endo_201111.jpg){kind=link}




Such a well researched piece.